
Urinary tract refers to the system that is concerned with formation storage and excretion of urine. It consists of two kidneys that lie at the back of upper part of abdomen, one on each side
Urine formed in the kidneys is drained by two hollow tubular structures, called the ureters into the bladder.
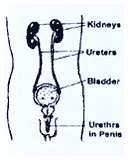
Bladder is a hollow muscular bag that lies in the lower part of abdomen. Bladder serves to hold urine tail it is full and then contracts to empty itself through another hollow tube called urethra, to the outside A muscular valve, called the sphincter, located in the urethra, keeps the urethra closed & opens when a person wishes to pass urine.
Depending upon the type and level of your injury, some functions of the bladder will be affected either temporarily or permanently. Some of the common changes that you may observe are
- Lack of sensation of
bladder fullness and/or
bladder fullness recognised by excessive sweating. flushing, tremors headache - Inability to judge urine leakage that occurs without one’s knowledge
- Inability to control passage of urine 4 Inability to pass urine at all or fully.
- Inability to pass urine at all or fully.
Depending upon neurological status, each person will observe ether one or various combinations of above mentioned symptoms. Neurological recovery takes a long time and this period may vary from few weeks to months to years. Therefore, the final behaviour pattern of bladder function will also take time to emerge
Immediately after SCI, the spinal is in a shock phase During this phase, there is complete inactivity of the bladder and its muscles are not capable of contraction Therefore, the bladder will continue to store large volumes of urine, becoming over distended. This state of over distention is detrimental for eventual bladder muscle recovery and imparts over stretching and thinning of its muscle Over distension prevented by an indwelling catheter placed in the bladder to keep it empty This n catheter is passed via the urethra and connected to a collection bag Between, ? 4 weeks when the spinal shock begins to wear, the indwelling catheter is removed and you will start doing intermittent catheterisation scheduled every 445 hours
Urine is stored in the bladder. As the bladder becomes full this information is passed via your spinal cord centres to your brain. If you wish to empty your bladder, then the bladder muscle contracts to empty the bladder.
Normally the desire can be modified. One can suppress the desire to pass urine until an appropriate time or place is available. Usually, the bladder empties completely leaving behind insignificant residue. Presence of large volume of urine at the end of voiding happens either because of weak muscles or some obstruction along the outlet
enerally there are two ways the bladder works after a spinal cord injury.
Spastic or Reflex Bladder means that when your bladder fills with urine, a reflex automatically triggers the bladder to empty. The problem in a reflex bladder is you do not know when the bladder will empty. Reflex or spastic bladder usually occurs when the injury is above the T12 level. The choice of bladder management methods for an individual with a spastic/reflex bladder include intermittent catheterisation, indwelling catheter and condon drainage.
Flaccid or non-reflex bladder means ones reflexes may be sluggish or absent. You may not feel when the bladder is full. It then becomes over distended and stretched. This can cause the urine to back-up through the ureters to the kidneys. Individuals with injuries below T12/L1 usually have a flaccid bladder. The bladder management system most commonly used is intermittent catheterisation. To avoid problem do not allow more than 400 cc of urine to fill in your bladder.
A bladder management programme allows you to plan for bladder emptying in an acceptable manner when it is convenient for you. This helps you to avoid accidents and prevent infections. Your level and type of injury will affect the choice you and your doctor make for your bladder programme. Because each person’s injury is different, your doctor will probably conduct some tests to see how your bladder functions. You also need to consider your hand function. How easy is it for you to do your own bladder programme? Can you manage alone or will you need help? During your rehabilitation you learn different ways to empty your bladder. The methods most frequently used are intermittent catheterisation; indwelling catheter; and the condon external catheter for male. You may use just one programme or a combination of methods. You will decide the method that works best for you. You can prevent leaking and have a pleasant outing by regulating your water intake Maintaining a voiding diary may help you plan A voiding diary is a statement of water intake Vs urine output in relation to time By analysing the diary, one can find out that by regulating the water intake at these trines, one can reduce my urine output a specified times to be comfortable.
Individuals with SCI are more likely to have urinary infection or other urinary problems with the urinary system. To avoid problems and keep you’re urinary system healthy.
Empty your bladder completely
After Your SCI your bladder often does not empty completely l?he residual ur ine becomes a breeding medium from bacteria and germs that may cause infection
Use a “clean technique” catheterisation
Always wash your hands before arid after doing catheterisation Be sure your catheter and equipment are clean Read the chapter on Clean Intermittent Catheterisation.
Keep skin clean and dry
Change your wet or soiled clothes immediately to avoid any bacterial growth n the genital area. Clean the area around the genitals with soap and water everyday.
Drink plenty of liquids
A steady intake of fluids helps “wash?out” bacteria and waste materials. Drinking the recommended amount of liquids helps avoid problems. How much fluid you need to drink each day depends on your bladder management. Water is the best fluid to drink.
Keep bladder pressures low
While you need to drink the recommended amount of fluid, you also need to empty your bladder on a regular schedule. Do not let more than 400cc of urine collect in your bladder anytime.
Loss of normal bladder function after spinal cord injury places you at a increased risk for urinary tract infection (UTI), regardless of the bladder management system you follow. Urinary tract infection can occur in the bladder, kidneys or other parts of the urinary tract.
The most common symptoms of bladder infection include going to the bathroom more frequently, passing blood in the urine. cloudy and odorous urine, increased spasticity in the lower extremities fever and chills Depending on your level of injury, you nay feel a burning with urination, or discomfort in the lower pelvis; area, abdomen or lower back.
If you notice any of these symptoms see the doctor for laboratory tests to determine the need for treatment. Research shows that UTIs that do not have symptoms usually do not need treatment with antibiotics. Use antibiotics only when symptoms (fever, chills and pain) are present. Your doctor based on your Urine Culture Report will prescribe antibiotics.
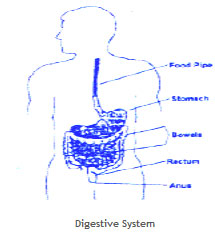 Losing bowel control with bowel accidents is probably the most embarrassing and frustrating experience that you have faced, as a result of your SCI. Proper bowel management is the answer to your problem. A bowel training program that aims at establishing a routine for emptying your bowels is the safest, most convenient and dependable for you. There is no single unfailing method that would suit everyone. Experimentation is needed in each case to find a method that suits one’s own needs and lifestyle Over a period of time the bowel can be ‘reeducated’ to empty regularly, adequately and at predictable times. The baseline for your program will be similar to the bowel pattern that you had before your injury. Even if you had an irregular bowel habit before your injury it is better to establish a more regular habit now as this will enable you to participate in a fuller social life without the fear of embarrassment of accidents.
Losing bowel control with bowel accidents is probably the most embarrassing and frustrating experience that you have faced, as a result of your SCI. Proper bowel management is the answer to your problem. A bowel training program that aims at establishing a routine for emptying your bowels is the safest, most convenient and dependable for you. There is no single unfailing method that would suit everyone. Experimentation is needed in each case to find a method that suits one’s own needs and lifestyle Over a period of time the bowel can be ‘reeducated’ to empty regularly, adequately and at predictable times. The baseline for your program will be similar to the bowel pattern that you had before your injury. Even if you had an irregular bowel habit before your injury it is better to establish a more regular habit now as this will enable you to participate in a fuller social life without the fear of embarrassment of accidents.
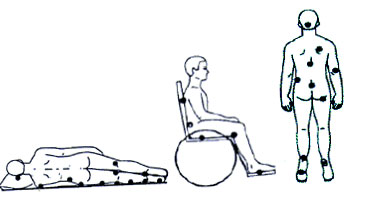 Parts of the body where skin and subcutaneous tissues that overlie bony prominence are likely sites for pressure sore formation. The parts where they form most often are shown in the picture. The points colored are the points of highest risk.
Parts of the body where skin and subcutaneous tissues that overlie bony prominence are likely sites for pressure sore formation. The parts where they form most often are shown in the picture. The points colored are the points of highest risk.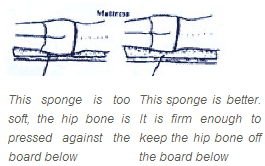 It is best to lie an a flat surface with a thick spongy mattress. A thick foam rubber mattress often works well. However some foam are so spongy that it sinks completely down under weight. Then the bony areas are no longer protected from pressure Therefore, the right mattress should be firm, thick and smooth.
It is best to lie an a flat surface with a thick spongy mattress. A thick foam rubber mattress often works well. However some foam are so spongy that it sinks completely down under weight. Then the bony areas are no longer protected from pressure Therefore, the right mattress should be firm, thick and smooth.
 If you can notice any of the danger signs, e.g. , redness, paleness, darkness, warmth or unnatural wrinkles over any susceptible points, then avoid pressure on that area until the warning signs disappear. This means not lying or sitting on that particular part.
If you can notice any of the danger signs, e.g. , redness, paleness, darkness, warmth or unnatural wrinkles over any susceptible points, then avoid pressure on that area until the warning signs disappear. This means not lying or sitting on that particular part.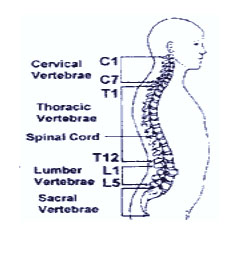 The backbone is the number one support for your body. The bones stacked on top of each other are called vertebrae and the spinal cord runs through them. The bones help protect the spinal cord. The vertebral column is made up of 33 bones called vertebrae. Seven vertebrae are in the neck region called Cervical Vertebrae denoted as C1, C2,C7, twelve in the thorax also called thoracic vertebrae and denoted as T1- T12 or D1-D12 and five in the lumbar region, L1- L5. There are five vertebrae in the sacral region (S1-S5) and remaining four are fused together as a vestigial organ, to remind us that our ancestors had tails. The spinal cord is a part of your nervous system. It is like a telephone wire that goes from your brain to the middle of your back, to your hips.
The backbone is the number one support for your body. The bones stacked on top of each other are called vertebrae and the spinal cord runs through them. The bones help protect the spinal cord. The vertebral column is made up of 33 bones called vertebrae. Seven vertebrae are in the neck region called Cervical Vertebrae denoted as C1, C2,C7, twelve in the thorax also called thoracic vertebrae and denoted as T1- T12 or D1-D12 and five in the lumbar region, L1- L5. There are five vertebrae in the sacral region (S1-S5) and remaining four are fused together as a vestigial organ, to remind us that our ancestors had tails. The spinal cord is a part of your nervous system. It is like a telephone wire that goes from your brain to the middle of your back, to your hips.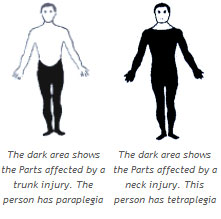 If you cannot move your legs but came move your arms like before, your spinal cord is hurt in your back (T1 and below) and you would be termed in medical language as a paraplegic.
If you cannot move your legs but came move your arms like before, your spinal cord is hurt in your back (T1 and below) and you would be termed in medical language as a paraplegic.
